


A video of the exiting nerve in a foramen found to be filled with scarring which did not show up on the MRI Scan. The disc wall is weak and the nerve was adherent to the disc wall. This is a typical finding
The maps of dermatomes and myotomes are derived from dissection studies of inert anatomy. The dysfunction such as numbness and weakness, have been used to determine the source of nerve compression in the spine. Inconveniently the makeup of the peripheral nerves does not always adhere to these conventions. The spinal; nerves may contain nerve fibres from adjacent levels or the construction of the plexus outside the spine, forming the peripheral nerve may vary in the selection of the nerve roots, termed “fixation”
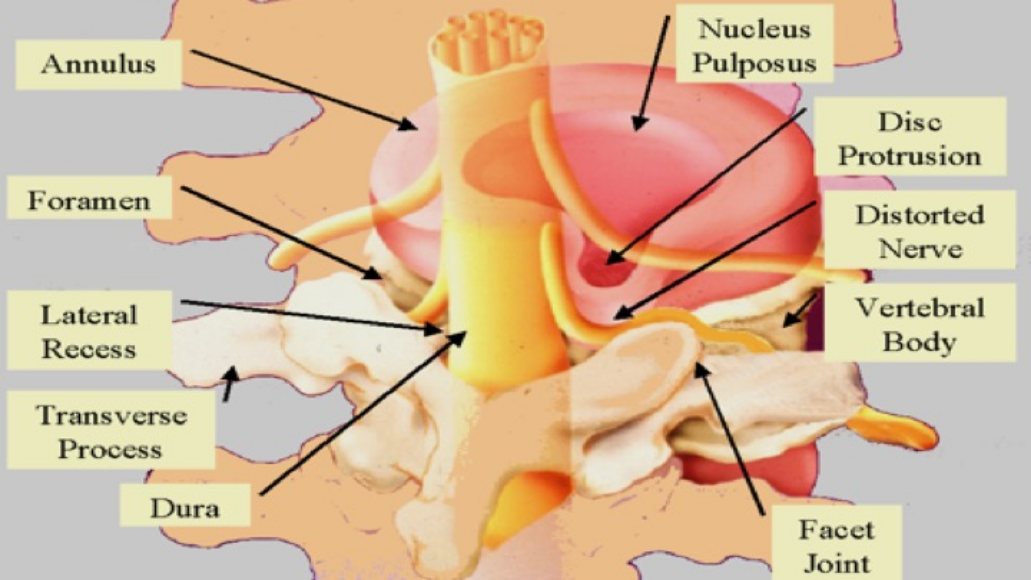
Each section consists of two adjacent vertebrae separated from the disc by a cartilaginous endplate. The disc consists of approximately 26 fibrous “onion” rings encircling a mobile hydraulic centre (Nucleus). The nerves descend from the brain as the spinal cord but at the level of the first lumbar vertebra (L1) they fan out as separate nerves likened to a Mare’s Tail (Cauda Equina), all being protected in a water jacket (Dura) filled with nutrient cerebrospinal fluid. The dura lies in in the spinal canal (Epidural Space) bounded by the disc in front, the facet joints on either side secured to the vertebrae by pillars of bone (Pedicles). Across the back of the space is an arch of bone (Lamina) bound to its neighbour by fibrous tissue termed the Yellow Ligament (Ligamentum Flavum). On either side at each level a spinal nerve leaves the epidural space through a tunnel (Foramen) to service the skin (Dermatome) and muscles (Myotome) related to that level. Look at the exiting nerve after clearance of much of the scarring in the foramen around the nerve
The facet joints are often attributed as a significant source of spinal pain and treated with injections and radiofrequency ablation of the posterior nerves that supply them. However their contribution to pain production may in fact be indirect. As the discs degenerate and loose height so the sliding surfaces slide over and impact on the nerve. The pain reaction causes spasm and increases the impaction. The injections and radiofrequency ablation reduces that spasm, overriding and impaction and so reduces the pain. Understandably the clinicians assume the pain came just from the facet joint. That said, arthritic facet joints can themselves cause pain but our experience suggests that the facet overgrowth can limit movement and so reduce the pain from the joint
The maps of dermatomes and myotomes are derived from dissection studies of inert anatomy. The dysfunction such as numbness and weakness, have been used to determine the source of nerve compression in the spine. Inconveniently the makeup of the peripheral nerves does not always adhere to these conventions. The spinal; nerves may contain nerve fibres from adjacent levels or the construction of the plexus outside the spine, forming the peripheral nerve may vary in the selection of the nerve roots, termed “fixation”